Content Isn't King. It's the Entire Kingdom
Your medical brilliance is worthless if no one can find it online
Summary
Transformed Hopkins' digital authority
Turned fragmented healthcare content into a competitive advantage
Connected patients with life-changing expertise
Despite being a top medical institution, Johns Hopkins lagged behind Mayo Clinic and Cleveland Clinic in digital health. Their online presence was fragmented, inconsistent, and did not reflect their medical expertise.
The problem wasn't unique to Hopkins. Across healthcare, organizations invest millions in website redesigns while neglecting authoritative, accessible content that helps people make significant decisions.
The Authority Gap, Excellence Without Accessibility
When I first explored Johns Hopkins' digital landscape, I encountered a common pattern in healthcare. Brilliant physicians created websites showcasing their expertise, but overlooked what patients needed.
One department greeted visitors with high-definition surgery footage that would fascinate medical students but terrify patients. Another featured complex anatomical diagrams challenging second-year students. A third led with dense academic publications demonstrating research excellence but offering no practical guidance.
Each site reflected the doctors' expertise, but none reflected the patient's experience.
This wasn't just a design problem; it was eroding their competitive advantage. While their medical excellence remained unquestioned, their digital authority was slipping to more organized competitors.
Why Healthcare Content Transformations Fail
I've witnessed the same pattern after leading content transformations in organizations. An executive announces the need for better content. Teams hire consultants. Everyone makes presentations with colorful charts. Twelve months later, nothing has changed.
Three primary factors often derail these initiatives:
1. The politics are very challenging.
During a difficult meeting, a department chair asked.
"Why should I give up control of my content? My team knows our field better than anyone else."
He wasn't wrong. His department included pioneers who developed surgical techniques taught globally. But his perspective revealed a fundamental misunderstanding affecting healthcare content initiatives.
The question isn't about who knows the medicine best, but who can translate that expertise into something patients can use. It's about creating a system where brilliant minds focus on sharing knowledge rather than managing websites.
2. The Stakes Are Higher Than Many Realize
This wasn't a typical corporate website merger where the worst outcome might be a temporary dip in lead generation. We were dealing with content guiding significant healthcare decisions.
One wrong redirect or one lost treatment options page, and you're not just losing traffic, you're potentially impacting patient care. The technical complexity matched the ethical responsibility.
3. Most Projects Start With Technology, Not Strategy
Show a room of medical experts a CMS demo, and watch their eyes glaze over. Then, show them how Mayo Clinic is outperforming them in their expertise, and you have their full attention.
Most healthcare content projects start with platforms and templates rather than purpose and strategy. They focus on containers rather than their content.
Finding a New Path Forward
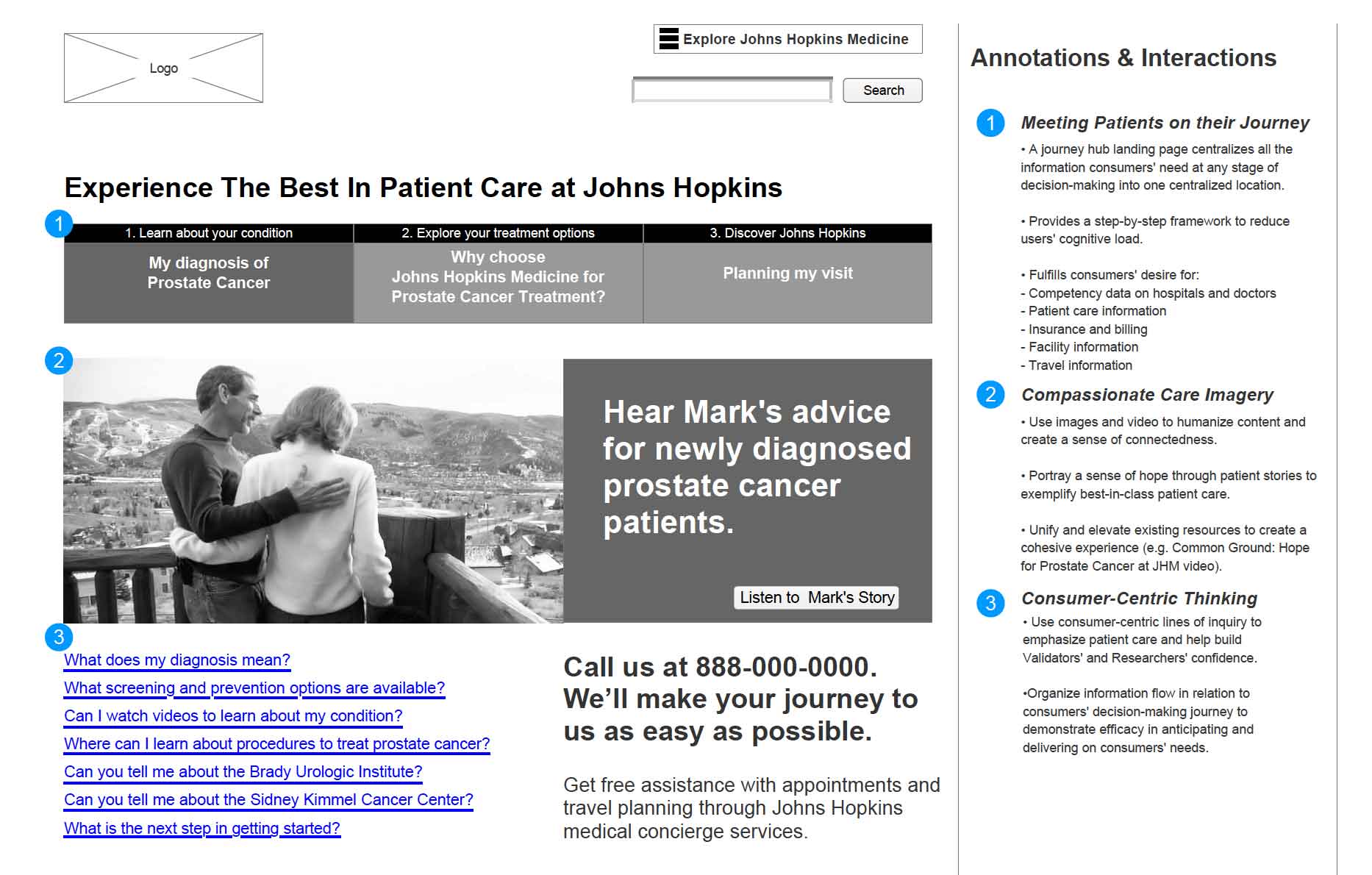
At Johns Hopkins, we took a different approach. We acknowledged the institution's unique strengths and the realities of patient behavior in the digital age.
Step 1: Map the Kingdom
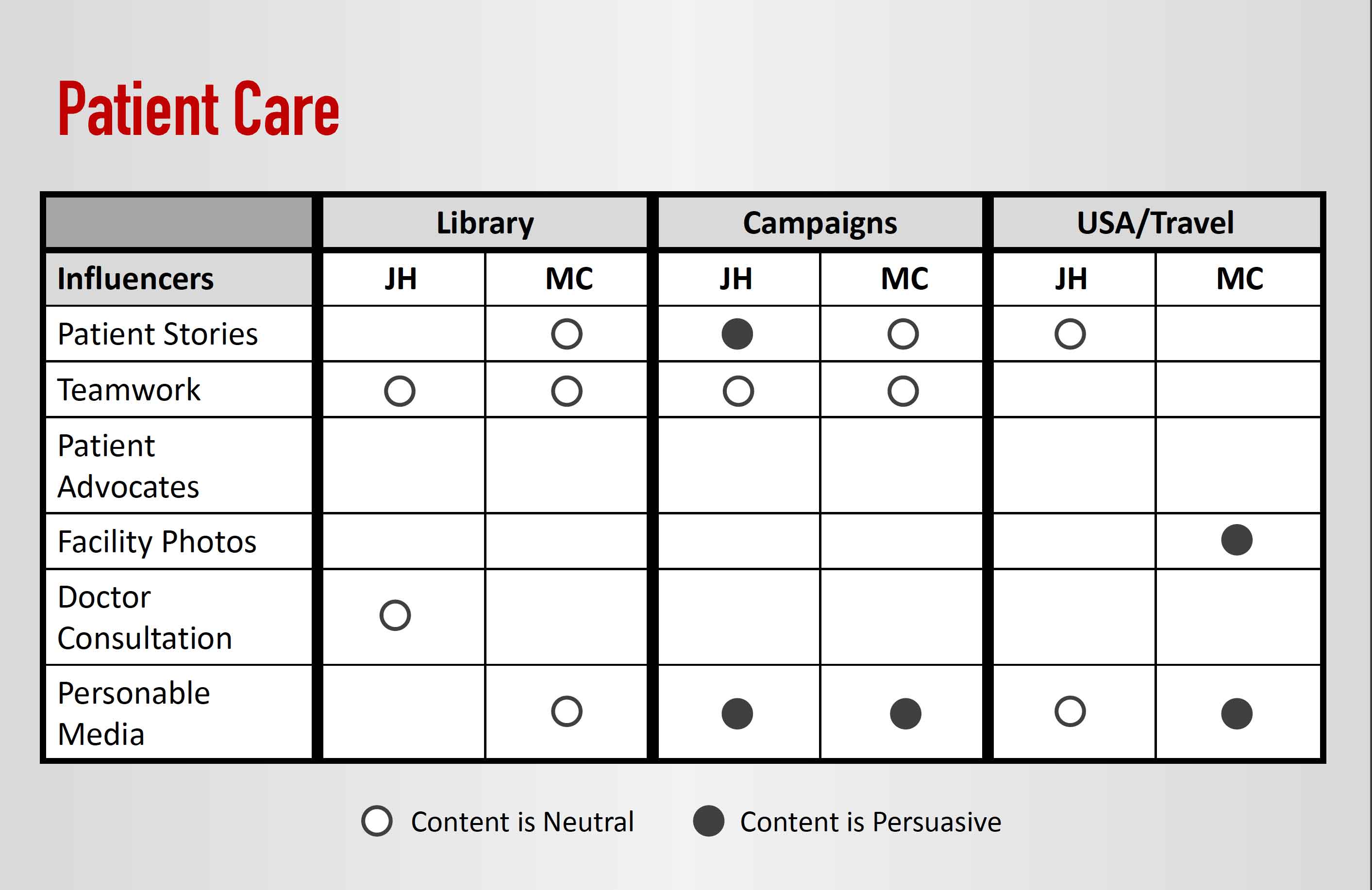
Instead of starting with solutions, we created a "content reality map" for each department. This wasn't just an inventory; it was a strategic assessment that showed:
- Where their content appeared in search results.
- How does it compare to competitors covering the same conditions?
- Where they had contradictory or duplicative information.
- Which content helped patients make choices?
The results were surprising for even the most digitally savvy departments. Pages they considered crucial had zero traffic, while forgotten content from years ago received thousands of monthly views.
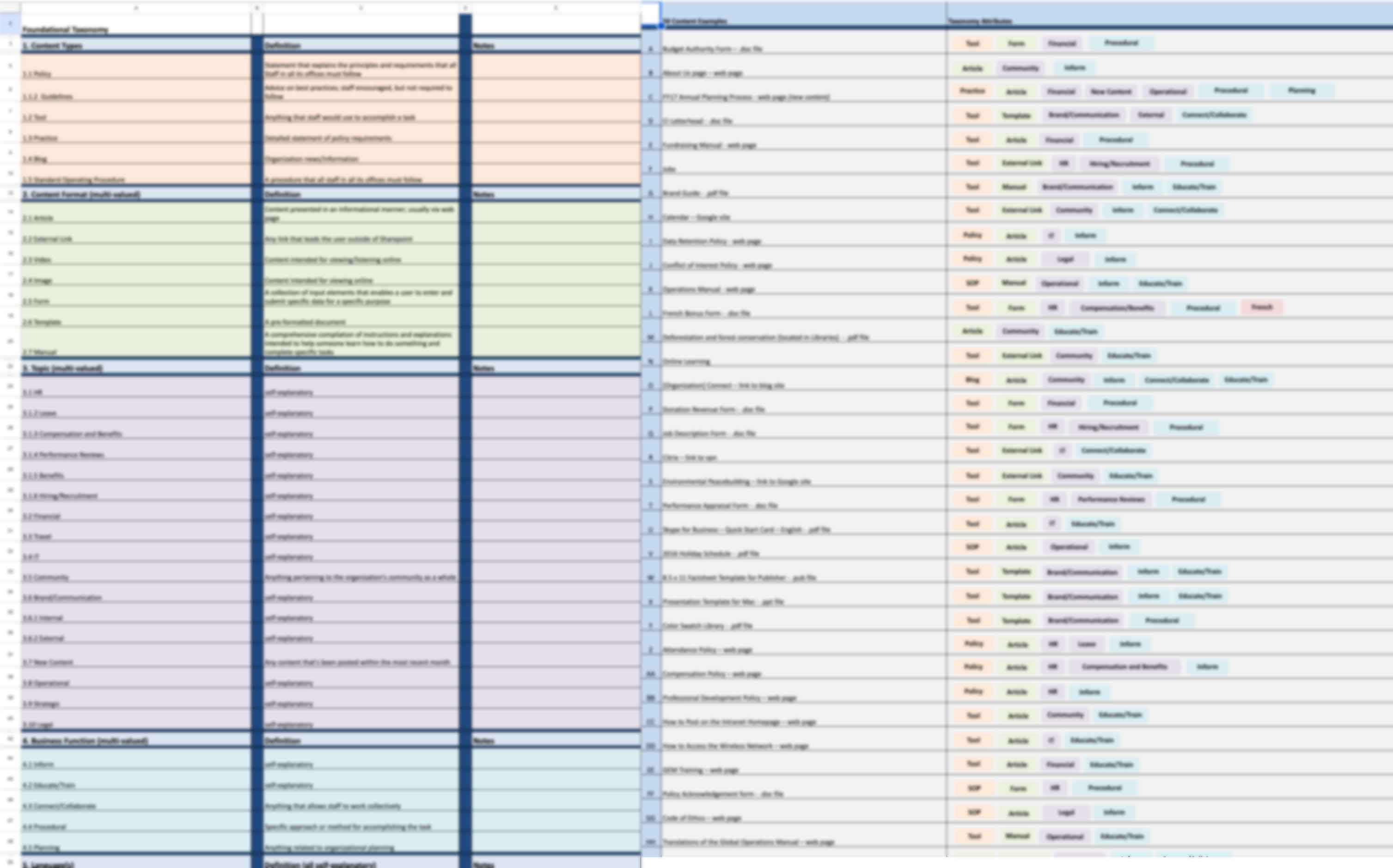
Step 2: Build the Foundation
Most content projects fail because they start with templates. We began with a modular architecture built around essential information units:
- Condition pages captured symptoms, causes, and treatments.
- Treatment pages outlined procedures, recovery expectations, and risks.
- Doctor profiles showcased expertise, research interests, and publications.
This wasn't just about organization. It was about scaling expertise. When a doctor updates a treatment description, it updates everywhere, eliminating contradictions and outdated advice across the digital ecosystem.
Step 3: Win Support Through Strategic Partnership
Instead of positioning departments as content contributors, we established them as strategic partners. For each clinical area, we demonstrated:
- How unified content would enhance rather than diminish their expertise
- Where they were losing ground to competitors in their specific areas
- How much time would centralized content management save teams?
- What they could achieve with that reclaimed time
Step 4: Migrate With Care
The migration process is the most technically challenging aspect of content transformation. One wrong move could impact years of built search rankings connecting patients to care.
We developed a "safety net migration system":
- Every URL had three confirmed mapped destinations.
- SEO specialists monitored rankings daily.
- Old pages stayed live until new ones demonstrated their value.
- Each department had a contingency plan for declining performance.
The approach was flawless.


Designing how expertise flows from those who have it to those who need it
From Content Chaos to Digital Authority
The transformation results extended beyond improved website metrics. The entire relationship between the institution and its digital presence evolved:
Doctors Became Educators, Not Website Managers
Instead of managing websites, medical experts could focus on sharing knowledge. They redirected the time spent on digital administration to creating valuable content.
One surgeon now dedicated nearly three hours weekly to creating patient education videos that reached thousands instead of a few.
Content Became a Competitive Edge
The analytics indicated the strategy was effective:
- Medical search visibility for key conditions increased.
- Organic traffic grew steadily quarter over quarter.
The most significant change was qualitative. Johns Hopkins began reclaiming its position as a medical and digital health authority meeting patients where they sought information.
The Bigger Truth About Healthcare Content
Most healthcare organizations misunderstand content strategy. They think it's about websites and text.
It's not.
It's about unlocking expertise, helping brilliant people reach more patients, and transforming content management into an advantage.
When done right, content strategy builds a better website and a stronger institution. It creates a system where knowledge flows freely from those who have it to those who need it.